Tick Bites and Diseases
Dan Onion, MD, MPH
Mt. Vernon/Vienna Health Officer
293-2076; dkonion@gmail.com
June, 2019
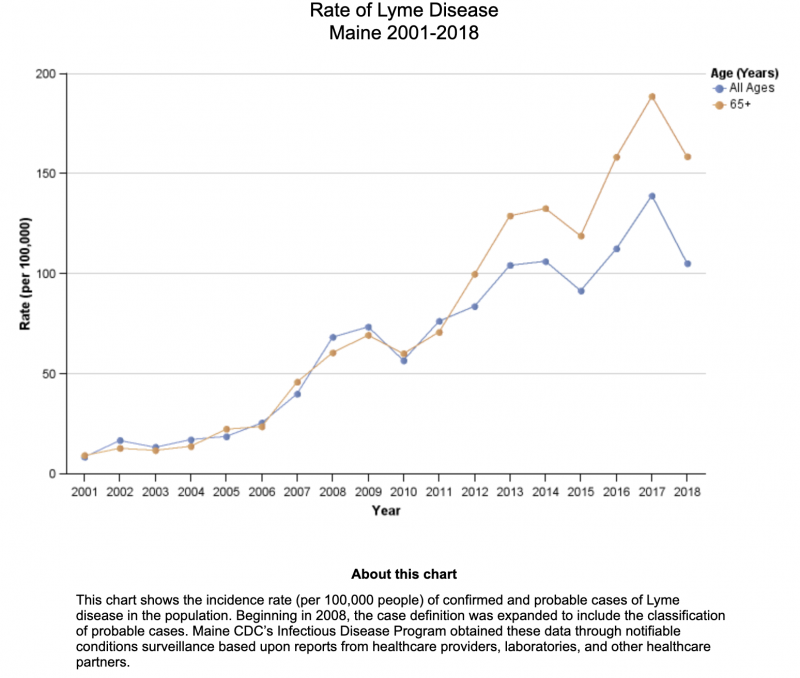
I just pulled the 5th tick of the year off my leg last night! It hadn’t embedded yet; rather it was racing up my leg to hide, tripping over my hairs and so alerting me. It reminded me that I haven’t written about ticks and the diseases they transmit in these columns since 2013! Time to review again, given that circumstances have worsened since then (Fig. 1).
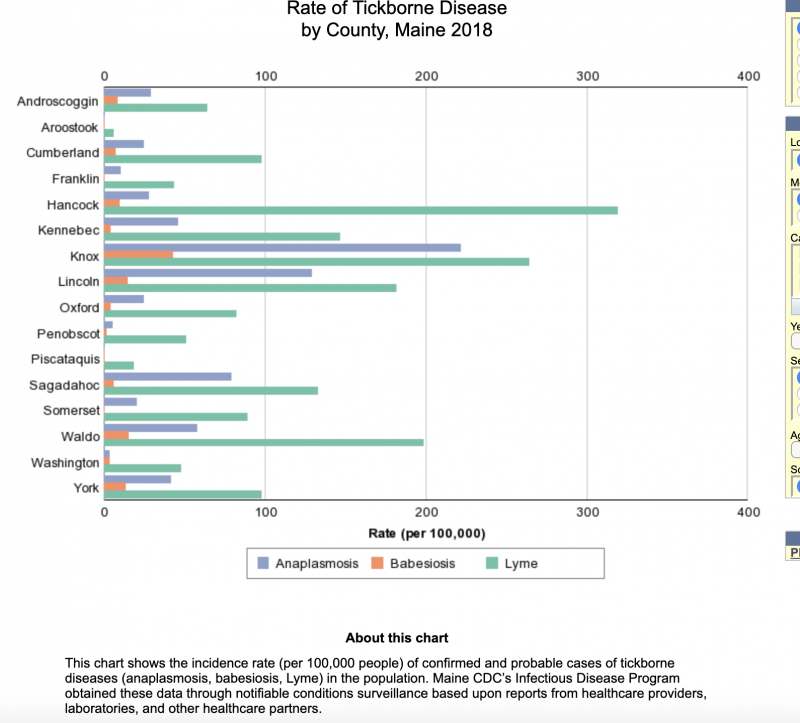
Deer ticks cause Lyme disease by transmitting Lyme bacteria when they attach to their animal/human victim. They can also transmit the less common diseases (Fig. 2), anaplasmosis and babesiosis, and rarely several others (ehrlichiosis, rocky mountain spotted fever, and others Maine used to be on the edge of the deer tick/Lyme disease infestation area, the southern New England states. But with long term warming and less winter kill, ticks and deer populations have increased substantially, so it is now much more common to see tick bites and consequently increased Lyme disease incidence, especially along mid-coast Maine (Fig. 3).
Lyme disease gets its name from the coastal town of Lyme, Connecticut. In 1975, a woman reported to Yale researchers 51 local cases of pediatric arthritis, which they identified and named “Lyme arthritis". In 1979, the name was changed to "Lyme disease" when other researchers discovered additional symptoms linked to the disease, including neurological problems and severe fatigue. In 1982 the bacteria causing the disease was discovered by Dr. Willy Burgdorfer, hence its name: Borrelia burgdorferi.
There are two common types of ticks here in Kennebec County: deer ticks, 5% of which are carriers of Lyme disease, and benign dog ticks. Deer ticks are half the size of apple seed-sized dog ticks, and lack the latters” white "racing stripes" down their backs. However, deer tick nymphs (babies), are more common this time of year, and are as small as poppy seeds, that is until they attach to people or animals and fill with blood to 10 times that size over several days. The longer a deer tick stays on, the more likely people are to contract Lyme disease, if the tick is a carrier. If they embed for fewer than 24-48 hours, disease rarely follows; most patients with Lyme disease have had a tick on for nearly a week.
Three to thirty days after a bite, the first sign of disease is usually a circular (usually over 3 inches in diameter), non-tender rash, called erythema chronicum migrans (EM), which looks like a red "ringworm" rash around a bull’s-eye bite site. The rash occurs in 70- 80% of patients. In Maine, EM is reported in just over 50% of patients. But don’t be alarmed about the small mosquito bite-like red spot appearing at the site of the bite itself within a day or two; it just reflects the bite injury, not a Lyme infection. Fever in 60% of patients, aching body and joints (90 + %), and headache (65%) also occur as the rash reaches its peak and begins to fade. If not treated, complications involving heart, nerves, brain, and joints can occur weeks and months later. Children 5-14 and people over 65 have these the most frequently. However, Lyme disease is almost never fatal, unlike the other rarer tick-borne diseases.
So how can you avoid these troubles without moving to Northern Canada? First, the most important thing to do is use DEET-containing bug dope to discourage their climbing on you, and tucking your pantlegs into your sox, a popular new Maine fashion now. Secondly, you should check yourself and your family for ticks daily if they’ve been outside whenever the ground isn’t frozen. This can be hard on parts of the body difficult to see, like the back side of your knees or trunk. I thought I'd grown a big skin tag behind my knee for several days, until I looked with a mirror and saw it was an engorged (swollen) tick not a big blueberry! Yikes! And wash, or at least heat in a dryer, clothes worn outside that may or do have ticks on them. Keeping your lawn mown may help by giving ticks less chance to climb up higher to jump on you; and some say light colored clothing helps, but I doubt the evidence basis for that.
If you find a tick, it's not swollen, and you are pretty sure it hasn't been on for more than a couple days, there is no need to submit it to the state lab for identification or be treated; just remove it and your chances of developing disease are very small. Slow steady pressure to pull it off usually works. The best instrument for this is a “tick spoon”, a baby spoon sized tool with a split down the middle to scoop up the trapped tick. Use tweezers to pull steadily but gently for the several minutes it takes to get the tick to release; I prefer a Leatherman for the revenge satisfaction. Breaking the head off in the bite leaves some, though substantially less, risk of infection. Don't try to burn the tick off; it may be tougher than your body will tolerate.
If the tick is engorged and may have been on for several days, then call your doctor/clinician for a single preventive dose of doxycycline. It will reduce your chances of getting Lyme from an infected tick from 3% to 0.6%.
If you develop the ring rash around the bite site weeks later, or in a place where you weren't aware you'd been bitten, then you should be given a course of antibiotics for 2-3 weeks, doxycycline/tetracycline for most, amoxicillin or cefuroxime for pregnant women and children, in whom the tetracyclines are not safe. The downside of the latter alternative antibiotics is that they don't also cover the rare co-infections with ehrlichiosis, anaplasmosis, and babesiosis. You will probably need to see a doctor/clinician to evaluate any such rash; ask for an urgent appointment. Sooner rather than later treatment is important. The rare, late complications are also treated with antibiotics after being proven due to Lyme by blood test immune titers.
So, use bug dope. Check yourself and the kids. Pull ticks off before they get engorged. And get antibiotics if you develop the characteristic rash or other symptoms.
For more information about ticks and many other public health risks, check out the Maine CDC portal here and their great section on ticks : here